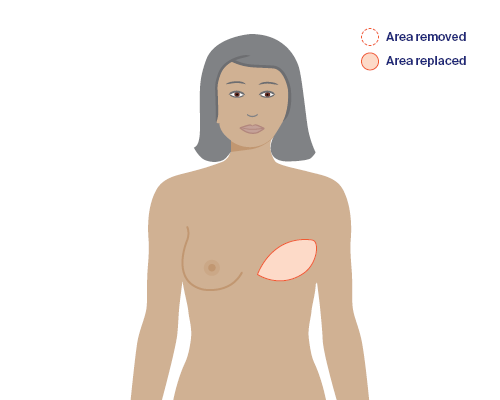
The shape of a breast can be built using your own muscle, fat and skin, which is taken from another area of the body. This is called a flap or autologous reconstruction.
Learn more about:
- Overview
- Location of flap reconstructions
- What to consider – flap reconstruction
- Flap from the lower abdomen
- Flap from the back (LD flap reconstruction)
- Less common types of flap procedures
- Risks of having a flap reconstruction
Overview
There are different types of flap reconstructions. Most use a flap of tissue from the tummy (abdomen). But tissue can also be taken from the back, bottom and thighs. See below for more details.
Your surgeon will discuss the type of flap reconstruction that is most suitable for you. This may depend on if you:
- have large breasts
- don’t have enough skin to cover an implant
- have had radiation therapy.
A flap reconstruction may not be suitable for you if you smoke; have diabetes, connective tissue disease or vascular disease; have had previous major abdominal surgery; or have a higher BMI.
There are benefits and drawbacks to having a flap reconstruction. You need to discuss these with your surgeon. They can also tell you how long the operation will take and the expected length of your recovery.
Location of flap reconstructions
The tissue for reconstructing your breast can come from different places. Your doctor will discuss the best location with you.
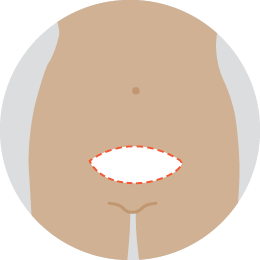 | DIEP flap Takes skin and fat but no muscle, from the lower abdomen. |
 | TRAM flap Takes skin, fat and muscle from the lower abdomen. |
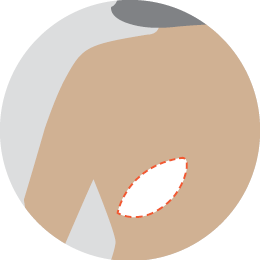 | LD flap Takes skin, fat and muscle from the back. |
Less common flap reconstruction
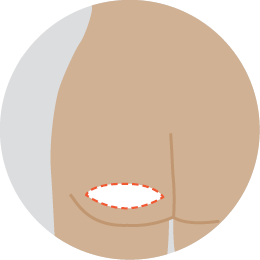 | SGAP or IGAP flap Takes fat and skin from the upper or lower bottom. |
 | TMG or TUG flap Takes skin, fat and a small amount of muscle from the upper inner thigh. |
 | PAP flap Takes fat, skin and muscle from the back of the upper thigh. |
Because I’d had extensive radiation therapy to the chest area, I was only suitable for a flap reconstruction. My reconstructed breast is absolutely amazing. It’s very symmetrical and even.
Lesley
→ READ MORE: What to consider – flap reconstruction
Key resource
Download a PDF booklet on this topic.
More resources

Dr Jane O’Brien, Specialist Oncoplastic Breast Cancer Surgeon, St Vincent’s Private Hospital, VIC; Clare Bradshaw, Clinical Nurse Consultant, Breast Assessment Unit, Fiona Stanley Hospital, WA; Rene Hahn, Consumer; Sinead Hanley, Consumer; Dr Marc Langbart, Specialist Plastic and Reconstructive Surgeon, Randwick Plastic Surgery, NSW; Melanie Law, Consumer; Sally Levy, Consumer; Annmaree Mitchell, Consumer; Ashleigh Mondolo, Breast Cancer Nurse Clinical Consultant, Mater Private Hospital Brisbane, QLD; Rochelle Osgood, Clinical Nurse Consultant – McGrath Breast Care Nurse, Sunshine Coast University Hospital, QLD: Dr Kallyani Ponniah, Head of Department, Breast Centre, Sir Charles Gairdner Hospital, WA; Meg Rynderman OAM, Consumer; Sarah Stewart, Breast Care Nurse, The Royal Women’s Hospital, VIC; Erin Tidball, 13 11 20 Consultant, Cancer Council NSW; Jane Turner, Senior Exercise Physiologist, Sydney Cancer Survivorship Centre, Concord Cancer Centre, NSW.
View the Cancer Council NSW editorial policy.