Oesophageal cancer begins when abnormal cells develop in the innermost layer (mucosa) of the oesophagus. A tumour can start anywhere along the oesophagus.
Learn more about:
- What is oesophageal cancer?
- Rare types of oesophageal cancer
- Who gets oesophageal cancer?
- What causes oesophageal cancer?
- GORD and Barrett’s oesophagus
- The oesophagus
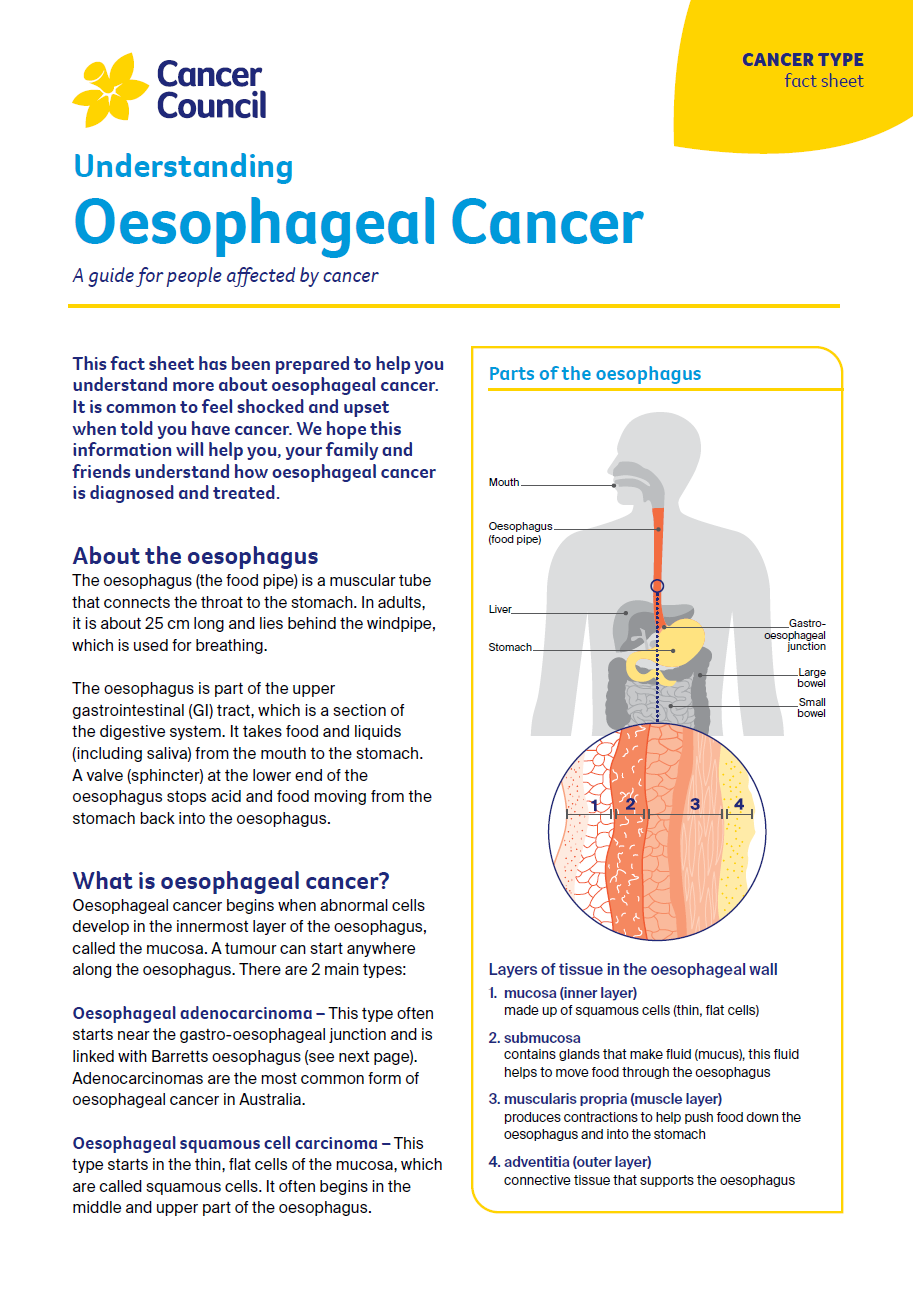
What is oesophageal cancer?
Oesophageal cancer begins when abnormal cells develop in the innermost layer of the oesophagus,
called the mucosa. A tumour can start anywhere along the oesophagus.
There are two main types:
Oesophageal adenocarcinoma – This type often starts near the gastro-oesophageal junction and is linked with Barrett’s oesophagus. Adenocarcinomas are the most common form of oesophageal cancer in Australia.
Oesophageal squamous cell carcinoma – This type starts in the thin, flat cells of the mucosa, which are called squamous cells. It often begins in the middle and upper part of the oesophagus.
Another type is gastro-oesophageal junction cancer.
This starts where the oesophagus meets the stomach. It is usually treated like oesophageal cancer, but sometimes like stomach cancer.
If not found and treated early, oesophageal cancer can spread to nearby lymph nodes or to other parts of the body (e.g. liver and lungs). It can also grow through the oesophageal wall and into nearby organs.
Rare types of oesophageal cancer
Other types of tumours can start in the oesophagus. These include small cell carcinomas, lymphomas, neuroendocrine tumours and gastrointestinal stromal tumours.
These types of cancer aren’t discussed here and treatment may be different. For more information, call Cancer Council 13 11 20.
Who gets oesophageal cancer?
In Australia, about 1785 people are diagnosed with oesophageal cancer each year. Men are almost
3 times more likely than women to be diagnosed with this cancer. It is more common in people over
60, but it can occur at any age.
What causes oesophageal cancer?
The exact causes of oesophageal cancer are not known. However, certain factors can increase the
risk. Many people with these risk factors do not develop oesophageal cancer. The risk factors are
different for oesophageal adenocarcinoma and oesophageal squamous cell carcinoma.
Known risk factors for oesophageal cancer include:
Oesophageal adenocarcinoma
- being overweight or obese
- medical conditions, including gastro-oesophageal reflux disease (GORD) and Barrett’s oesophagus
- smoking tobacco
- being over 60
Oesophageal squamous cell carcinoma
- drinking alcohol
- smoking tobacco
- being over 60
- damage to the oesophagus from swallowing very hot liquids or corrosive substances (e.g. acid).
GORD and Barrett’s oesophagus
Reflux occurs when stomach acid flows up into the oesophagus. When reflux happens over a long time, it can lead to gastro-oesophageal reflux disease (GORD).
Over time, acid and bile can damage the oesophagus lining, causing inflammation or ulcers
(oesophagitis). This can lead to Barretts oesophagus, which affects about 1 in 10 people with GORD.
Rarely, Barretts oesophagus can develop into oesophageal adenocarcinoma (see previous page). If you have Barretts oesophagus, your doctor may recommend regular endoscopies.
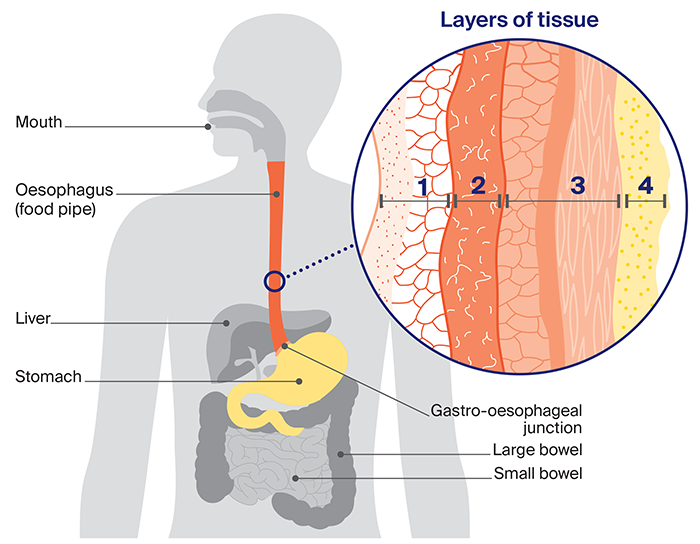
The oesophagus
The oesophagus (the food pipe) is a muscular tube that connects the throat to the stomach. In
adults, it is about 25 cm long and lies behind the windpipe, which is used for breathing.
What the oesophagus does
The oesophagus is part of the upper gastrointestinal (GI) tract, which is a section of the digestive system. It takes food and liquids (including saliva) from the mouth to the stomach.
A valve (sphincter) at the lower end of the oesophagus stops acid and food moving from the
stomach back into the oesophagus.
Layers of tissue in the oesophageal wall |
|
|
1. mucosa |
|
|
2. submucosa |
|
|
3. muscle propria |
|
| 4. adventitia (outer layer) |
|
Anatomy of the oesophagus
→ READ MORE: Oesophageal cancer symptoms
Key resource
Download a PDF booklet on this topic.
More resources

Prof David Watson, Matthew Flinders Distinguished Professor of Surgery, Flinders University, and Senior Consultant Surgeon, Oesophago-Gastric Surgery Unit, Flinders Medical Centre, SA; Prof Bryan Burmeister, Senior Radiation Oncologist, GenesisCare Fraser Coast and Hervey Bay Hospital, QLD; Dr Natalie Collier, Radiation Oncologist, Wollongong Hospital, NSW; A/Prof Melissa Eastgate, A/Executive Director, Cancer Care Services, Royal Brisbane and Women’s Hospital, QLD; Natalie Lalor, 13 11 20 Consultant, Cancer Council Victoria; Chris Menzies, Upper GI Cancer Nurse Consultant, Flinders Medical Centre and Southern Adelaide Local Health Network, SA; Tammy Milne, Consumer; Stefanie Simnadis, Clinical Dietitian, St John of God Subiaco Hospital, WA; Prof Rajvinder Singh, Professor of Medicine, University of Adelaide, and Director, Gastroenterology Department and Head of Endoscopy, Lyell McEwin Hospital, SA.
View the Cancer Council NSW editorial policy.