People with early NSCLC (stage 1 or 2) will generally be offered surgery to remove the tumour.
Learn more about:
- Overview
- Types of lung surgery
- Removing lymph nodes
- How the surgery is done
- What to expect after surgery
Overview
How much of the lung is removed depends on several factors:
- the location and size of the cancer
- your general wellbeing and fitness
- how your lungs are working (lung function).
Surgery is not suitable for most people with advanced lung cancer.
If there is fluid in the pleural cavity (called pleural effusion) that keeps returning, you may have surgery (pleurodesis) to control this, or need to insert a catheter. Read more on this procedure.
Types of lung surgery
Surgery for lung cancer may remove all or part of a lung.
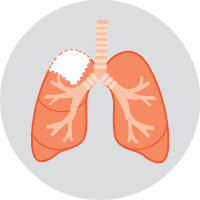
 | LobectomyThis is the most common type of surgery for lung cancer. In a lobectomy, one of the lobes of the lung (about 30–50% of the lung) is removed. |
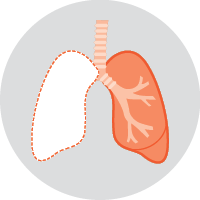 | PneumonectomyIf the cancer is in more than one lobe of a lung, or near where the airways enter the lung, a pneumonectomy may be done. In this operation, a whole lung is removed. It’s possible to still breathe normally with one lung. |
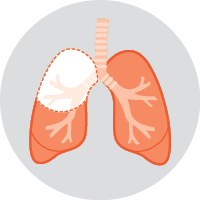
  | SegmentectomyFor some early-stage lung cancers that are on the edge of the lung, a segmentectomy may be used. In this operation, a small part of the lobe is removed. In cases where a patient is very unwell, however, a wedge resection may be considered. A wedge resection removes only a tiny piece of the lobe. |
Many hospitals in Australia have programs to reduce the stress of surgery and improve your recovery. Called enhanced recovery after surgery (ERAS) or fast-track surgical (FTS) programs, they provide information about what to expect each day after surgery. Read more information about preparing for treatment.
Removing lymph nodes
During surgery, the lymph nodes near the cancer will also be removed to check whether the cancer has spread. Knowing if the cancer has spread to the lymph nodes helps the doctors decide whether you need further treatment with chemotherapy or radiation therapy.
How the surgery is done
There are 2 main ways to perform surgery for lung cancer, and both require a general anaesthetic. Each type of surgery has advantages in particular situations – talk to your surgeon about the best option for you.
VATS
Lung cancer surgery can often be done using a keyhole approach. This is known as video-assisted thoracoscopic surgery (VATS). The surgeon will make a few small cuts (incisions) in the chest wall.
A tiny video camera and operating instruments are passed through the cuts, and the surgeon performs the operation from outside the chest. A keyhole approach usually means a shorter hospital stay, faster recovery and fewer side effects.
Thoracotomy
If a long cut is made between the ribs in the side of the chest, the operation is called a thoracotomy. This may also be called open surgery. You will need to stay in hospital for 3–7 days.
Sometimes the surgeon may need to change from a VATs approach to a thoracotomy during the surgery.
See our general section on Surgery for more information about surgery and recovery.
→ READ MORE: What to expect after surgery
Podcast: Making Treatment Decisions
Listen to more of our podcast for people affected by cancer
Dr Malinda Itchins, Thoracic Medical Oncologist, Royal North Shore Hospital and Chris O’Brien Lifehouse, NSW; Dr Cynleen Kai, Radiation Oncologist, GenesisCare, VIC; Dr Naveed Alam, Thoracic Surgeon, St Vincent’s Hospital, Epworth Richmond, and Monash Medical Centre, VIC; Helen Benny, Consumer; Dr Rachael Dodd, Senior Research Fellow, The Daffodil Centre, NSW; Kim Greco, Specialist Lung Cancer Nurse Consultant, Flinders Medical Centre, SA; Caitriona Nienaber, 13 11 20 Consultant, Cancer Council WA; Marco Salvador, Consumer; Janene Shelton, Lung Foundation Australia – Specialist Lung Cancer Nurse, Darling Downs Health, QLD; Prof Emily Stone, Respiratory Physician, Department of Thoracic Medicine and Lung Transplantation, St Vincent’s Hospital Sydney, NSW; A/Prof Marianne Weber, Stream Lead, Lung Cancer Policy and Evaluation, The Daffodil Centre, NSW.
View the Cancer Council NSW editorial policy.