For some people, surgery may be the only treatment needed.
Learn more about:
- Overview
- Types of surgery
- How the surgery is done
- What to expect after surgery
- Side effects of surgery
- Taking care of yourself at home
Overview
Surgery is usually recommended when the tumour is in the cervix only. The type of surgery you have will depend on how far within the cervix the cancer has spread. See the images below for more information about the main types of surgery.
Learn more about surgery.
If becoming a parent is important to you, talk to your doctor before starting treatment and ask for a referral to a fertility specialist. Learn more about fertility and cancer.
Types of surgery
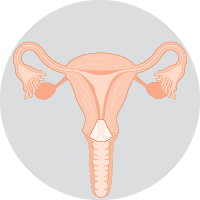 | Cone biopsyRemoves a cone-shaped piece of tissue around the cancer, including a margin of healthy tissue. A cone biopsy is used to treat very early cervical cancers. Learn more about the cone biopsy. |
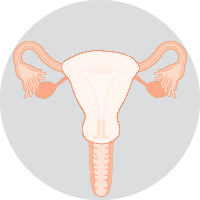 | Total hysterectomyRemoves the uterus and cervix. This surgery is used for early cervical cancer. The fallopian tubes are often removed too. If you haven’t gone through menopause, you may be able to keep your ovaries. |
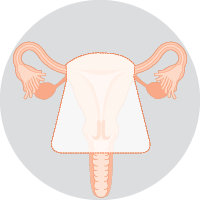 | Radical hysterectomyRemoves the uterus, cervix, and top of the vagina. This is the usual surgery for most cervical cancers. The fallopian tubes are often removed as well. You may be able to keep your ovaries if you have not gone through menopause. |
 | Bilateral salpingo-oophorectomyRemoves both fallopian tubes and ovaries. This may be done during a hysterectomy if there is a risk the cancer has spread, or if you have been through menopause. |
![]()
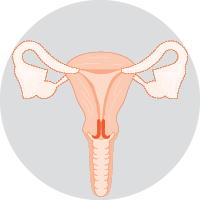
Lymph node surgery
Lymph nodes in the pelvis or groin may be removed to check for the spread of cancer. This is called a lymphadenectomy (lymph node dissection).How the surgery is done
The surgery is done under a general anaesthetic. Research has shown that outcomes are generally better with open surgery (laparotomy). This means that the surgery is performed through a cut in the abdomen.
Keyhole surgery (laparoscopy or robotic surgery) may be used for selected cases, usually early cervical cancer. Your surgeon will talk to you about the most suitable surgery for you, as well as any risks.
→ READ MORE: What to expect after surgery
Podcast: Making Treatment Decisions
Listen to more episodes from our podcast for people affected by cancer
More resources

Dr Antonia Jones, Gynaecological Oncologist, Royal Women’s Hospital and Mercy Hospital for Women, Melbourne, VIC; Angelyn Aligarbes, Consumer; A/Prof Emma Allanson, Gynaecological Oncologist and Head of Dept, Gynaecologic Oncology, King Edward Memorial Hospital for Women, WA; Gemma Busuttil, Radiation Therapist Specialist, Crown Princess Mary Cancer Centre, Westmead Hospital, NSW; Laura Carman, 13 11 20 Consultant, Cancer Council VIC; Danielle Carpenter, Gynaecology Nurse Consultant, Peter MacCallum Cancer Centre, VIC; A/Prof Pearly Khaw, Lead Radiation Oncologist – Gynae-Oncology, Peter MacCallum Cancer Centre, VIC; Georgina Richter, Gynae-Oncology Clinical Nurse Consultant, Royal Adelaide Hospital, SA; A/Prof Megan Smith, Research Fellow, Cancer Elimination Collaboration, University of Sydney, NSW; Sophia Wooldridge, Senior Clinical Psychologist, Hunter New England Centre for Gynaecological Cancer, John Hunter Hospital, NSW; Melissa Whalen, Consumer.
View the Cancer Council NSW editorial policy.