The type of operation you have depends on where in the rectum the cancer is, whether the bowel can be rejoined, and where in the rectum the join can be made. There are 2 main types of operation – an anterior resection or an abdominoperineal resection (which may also be called an abdominoperineal excision).
Anterior resection
This is the most common operation. You may have a high anterior resection or an ultra-low anterior resection (see below). As part of the procedure, the surgeon may create a temporary stoma (which will usually be reversed later). See more information about stomas.
Abdominoperineal resection
This procedure may be recommended if the cancer is near the anal sphincter or it is too low to be removed without causing incontinence (loss of control over bowel movements). After an abdominoperineal resection, you will need a permanent stoma (colostomy). See more information on having a stoma and speak to your surgeon about any concerns you may have.
Types of resections
There are different types of operations for cancer in the rectum. The surgery may be done as open or keyhole surgery.
 | High anterior resectionThe surgeon removes the lower left part of the colon and the upper part of the rectum. Nearby lymph nodes and surrounding fatty tissue are also removed. The lower end of your bowel is rejoined to the top of the remaining rectum. |
 | Ultra-low anterior resectionThe lower left part of the colon and all or part of the rectum are removed, along with nearby lymph nodes and surrounding fatty tissue. The end of the remaining bowel is joined to the lowest part of the rectum, just above the anus. In some cases, the surgeon may make a pouch using the remaining colon and join this pouch to the anus to improve ongoing bowel function. This is known as a colonic J-pouch. |
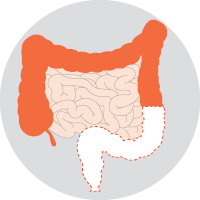 | Abdominoperineal resection or excision (APR or APE)The sigmoid colon, the entire rectum and the anus are removed. Your surgeon uses the descending colon to create a permanent stoma (known as a colostomy) for faeces to leave the body. The anal area will be stitched up and permanently closed. |

→ READ MORE: Other types of surgery for bowel cancer
Podcast: Coping with a Cancer Diagnosis
Listen to more of our podcast for people affected by cancer
More resources

Prof Alexander Heriot, Colorectal Surgeon and Director Cancer Surgery, Peter MacCallum Cancer Centre, Director, Lower GI Tumour Stream, Victorian Comprehensive Cancer Centre, VIC; Dr Cameron Bell, Gastroenterologist, Royal North Shore Hospital, NSW; Graham Borgas, Consumer; Prof Michael Bourke, Director of Gastrointestinal Endoscopy, Westmead Hospital, The University of Sydney, NSW; Laura Carman, 13 11 20 Consultant, Cancer Council Victoria, VIC; Amanda Connolly, Specialist Bowel Care Nurse, Icon Cancer Centre Windsor Gardens, SA; A/Prof Melissa Eastgate, Operations Director, Cancer Care Services, Royal Brisbane and Women’s Hospital, QLD; Anne Marie Lyons, Stomal Therapy Nurse, Concord Repatriation General Hospital and NSW Stoma Ltd, NSW; Lisa Nicholson, Manager Bowel Care Services, Bowel Cancer Australia, NSW; Stefanie Simnadis, Clinical Dietitian, St John of God Subiaco Hospital, WA; Rafi Sharif, Consumer; Dr Kirsten van Gysen, Radiation Oncologist, The Nepean Cancer and Wellness Centre, NSW; Sarah Williams, Clinical Nurse Consultant, Lower GI, Peter MacCallum Cancer Centre, VIC.
View the Cancer Council NSW editorial policy.